Scaphoid Non Union
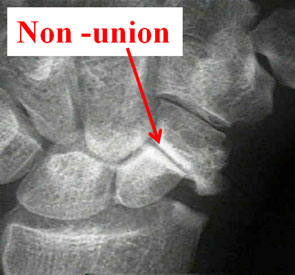 Because the scaphoid has a blood supply which comes from only one side it is prone to not healing. X-rays are routinely taken of the scaphoid as it heals; if it does not heal it is usually clear to see. Sometimes a scaphoid non union is found quite by chance when x-rays are taken of the wrist for other reasons. Usually because patients have injured their wrist many years before, did not attend hospital and a scaphoid fracture was never diagnosed or treated. Other times a scaphoid fracture appeared united on check x-rays but in fact still had a crack in it.
Because the scaphoid has a blood supply which comes from only one side it is prone to not healing. X-rays are routinely taken of the scaphoid as it heals; if it does not heal it is usually clear to see. Sometimes a scaphoid non union is found quite by chance when x-rays are taken of the wrist for other reasons. Usually because patients have injured their wrist many years before, did not attend hospital and a scaphoid fracture was never diagnosed or treated. Other times a scaphoid fracture appeared united on check x-rays but in fact still had a crack in it.
Non-unions can be pain free for a long time but may become troublesome many years after the injury. This is because they form what is called a 'fibrous non union' where the gap in the bone is filled with scar tissue which 'glues' the fracture together. Because the bone is stable it does not hurt and should not be interfered with. If it becomes painful surgery should be considered.
Surgery for scaphoid non union
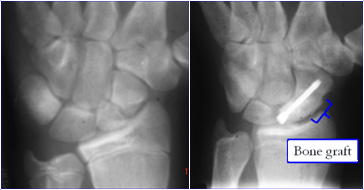 Surgery to treat a non union uses bone graft which may be taken from the hip or the radius. The bone used in grafting has lots of bone healing cells in it, when placed in the fracture site it helps the non-union to heal. When taken from the hip only a 1cm chunk of bone is removed, however the operation site is reported as being very painful for a few weeks. The wound and dressings should be treated in the same way as the wrist wound (see below). The non union site is cleaned back to healthy bleeding bone. The bone graft is then packed into the gap and held with a headless screw.
Surgery to treat a non union uses bone graft which may be taken from the hip or the radius. The bone used in grafting has lots of bone healing cells in it, when placed in the fracture site it helps the non-union to heal. When taken from the hip only a 1cm chunk of bone is removed, however the operation site is reported as being very painful for a few weeks. The wound and dressings should be treated in the same way as the wrist wound (see below). The non union site is cleaned back to healthy bleeding bone. The bone graft is then packed into the gap and held with a headless screw.
Avascular necrosis (AVN) - Vascularised bone grafting.
 This is the term given to bone which has died because it has not got a blood supply; typically affecting non union of a proximal pole fracture. The bone may look white on an x-ray or show up as dark on an MRI scan. Because the bone is dead it had 'turned to chalk' and is very difficult to get to heal. In this instance a vascularised bone graft may be used. This involves taking a piece of bone from the radius that unlike the bone graft used normally, has a small blood vessel feeding it. Next the small square of bone with the vessel and placing it is lifted into the non union site. In this way the blood supply is plumbed directly into the dead bone. Even with this advanced surgery the success rate of gaining a healthy united scaphoid in the presence of AVN is only 40-55%.
This is the term given to bone which has died because it has not got a blood supply; typically affecting non union of a proximal pole fracture. The bone may look white on an x-ray or show up as dark on an MRI scan. Because the bone is dead it had 'turned to chalk' and is very difficult to get to heal. In this instance a vascularised bone graft may be used. This involves taking a piece of bone from the radius that unlike the bone graft used normally, has a small blood vessel feeding it. Next the small square of bone with the vessel and placing it is lifted into the non union site. In this way the blood supply is plumbed directly into the dead bone. Even with this advanced surgery the success rate of gaining a healthy united scaphoid in the presence of AVN is only 40-55%.
What should I expect after surgery?
Local anaesthetic will be injected into the wound at the end of the operation. This area will remain numb for up to six hours after surgery. Before the effect wears off, you should take painkillers which should be taken on a regular basis. Swelling causes stiffness and pain which is made worse by hanging the arm down at your side or resting it on your lap. Swelling is best prevented by keeping the hand above the level of the heart for the first 48 hours. It is also important to keep the fingers moving through a full range of motion.
Your plaster will be removed at 2 weeks to check the wound. Your stitches are absorbable so they will not need to be removed. You will then be place in a light weight cast for a further 4 weeks. Once the plaster is removed, it is safe to get the hand wet. The wound and the surrounding skin often become very dry and will be more comfortable if a moisturiser is applied, including on the wound itself. Initially the scar will be thickened and tender to touch. This must be massaged firmly with a moisturising cream to reduce sensitivity and swelling. You will be placed in a splint which can be removed for hand exercises.
Is there anything that can go wrong?
Operations to fix the scaphoid are very successful and most people who have them are delighted with the operation and are glad they had it done. Like any operation a number of people can have a problem.
- Infection can occur after any operation and would be treated by antibiotics. If the hand becomes red, hot and very swollen you must go to your GP or ring your consultant's secretary.
- Even though the surgery gives the non union the best chance of healing there is about a 20% chance of the fracture failing to unite for the second time. This is more likely when there has been a long delay, you have had previous scaphoid surgery, fracture is at the proximal pole or if there is poor blood supply in the bone (see AVN).
- Your fracture should unite over a 6-8 week period but it can often be 3 months before you can return to heavy manual work. The fracture can take even longer to heal and patience may be required.
- Surgery attempts to prevent the development of arthritis; however it can still occur over a 2 to 10 year period.
- The scar will be a little firm to touch and tender for 6-8 weeks, neuromas can form which small tender areas caused tiny nerves under the skin. These can be removed easily.
- You are likely to lose movement at the wrist, usually 50% of the normal side.
- Very rarely the hand goes into shock as a reaction to the trauma of the surgery and the hand may become swollen, painful and stiff (Complex Regional Pain Syndrome). This problem cannot be predicted. The treatment is physiotherapy and sometimes injections are necessary. It gets better on its own bur can take many months.
You should discuss the possibility of problems with your surgeon before your operation.