Shoulder impingement
 What is shoulder impingement syndrome?
What is shoulder impingement syndrome?
Shoulder impingement is the collective name for pain which gets worse on lifting the arm out to the side. It is therefore a symptom of several conditions of the shoulder and the treatment will vary according to the cause. You should ask your surgeon what has caused your impingement symptoms before treatment begins.
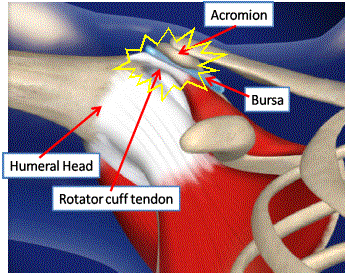
The pain comes from the tendon and the bursa (fluid filled sac) which both get trapped between one of the shoulder bones (humeral head) and the roof of the shoulder (Acromion). The impingement occurs because there is not enough space for the tendon to slide under the acromion on lifting the arm it becomes pinched, inflamed and sometimes torn.
Possible causes:-
- Tendonitis. The tendon becomes inflamed and swells. This means that it is too large for the gap between the acromion and the humeral head that results in rubbing as the tendon passes under the acromion as the arm is lifted. This in turn causes more inflammation and a vicious cycle develops of injury and swelling. Common in patients who perform repetitive over arm activities and swimmers. A steroid injection followed by physiotherapy is usually effective, however if symptoms persist then an arthroscopic sub acromial decompression will relieve the symptoms. This is a key hole procedure to remove all the inflamed tissue and bursa. A thin layer of bone is removed from under the acromion which causes a rich healing response and helps the tendon to heal. (see video - Subacromial decompression)
- Calcific tendonitis. Deposits of calcium collect in the cuff tendon. Not only is this irritating to the tendon but it also takes up space so there is a mechanical impingement as the tendon passes under the acromion on lifting the arm. This type of tendonitis is very painful and relief of symptoms can be achieved with a steroid injection into the sub acromial space. Unfortunately the steroid does not always give long term relief of symptoms and surgery in the form of arthroscopic debridement of the calcific deposit is required.
- Cuff tear. If the rotator cuff has a tear or partial tear the free ends will rub under the acromion. If the tear is large the cuff will not be able to pull the ball into the socket as the arm is lifted, consequently the humeral head bangs against the acromion. For more information on rotator cuff tear click here.
- Minor instability. If the ball is not centralised in the cup as the arm is lifted, the humeral head will drift upwards as the larger muscles (such as the deltoid) pull it towards the acromion. The causes of this minor instability can be poor muscle balance, loss of scapular control (winging or protraction) or even poor posture starting from the spine (core stability). This is the main cause of impingement in young patients and can usually be treated with specialist physiotherapy. For more information on shoulder instability click here.
- Bony spur. The acromion can be many shapes and some people have a spur. With age this can increase in size and start to rub on the tendon below. This can be treated with arthroscopic removal with a burr. see video - subacromial decompression
- Acromio-clavicular arthritis. This is a joint between the acromion and the clavicle (collar bone) when it becomes arthritic bone heaps up on the side of the joint. This heaped up bone (osteophytes) rubs on the underlying cuff tendon and cause impingement. see video - distal clavicle resection
What is done at surgery?
After a routine shoulder diagnostic arthroscopy a shaver is introduced into the sub acromial space and the bursa and underside of the acromion is removed with a burr. This removes the painful inflamed tissue and creates more space for the tendon in the shoulder joint. The surgery is done with an anaesthetic block so the arm will be numb, if you prefer you can be awake during the operation or have some sedation to make you sleepy. Because the operation uses water to see inside the joint the wounds will leak a little fluid which will be absorbed by cotton wool dressings, which are removed a few hours after surgery. You can go home the same day after seeing the ward physiotherapist who will give you exercises to do. see video- subacromial decompression.
What should I expect during recovery?
 Once the numbness has worn off (4-8 hours) the shoulder will become painful after the operation if you do not take regular pain killers as soon as you get home. Even though you may be pain free at rest you must take the tablets for when you move the shoulder as part of your rehabilitation program. A combination of regular painkillers such as paracetamol or codeine should be taken with NSAIDs (unless contra-indicated) such as ibuprofen- which is also an anti inflammatory drug. If the pain killers you have been given are not sufficient please contact your consultant's secretary or your GP. The little incisions are covered with a small sticky dressing which should be kept dry and replaced with spare dressings when necessary. You will be given these before leaving hospital. You will be given a sling which will protect your shoulder and help with pain relief.
Once the numbness has worn off (4-8 hours) the shoulder will become painful after the operation if you do not take regular pain killers as soon as you get home. Even though you may be pain free at rest you must take the tablets for when you move the shoulder as part of your rehabilitation program. A combination of regular painkillers such as paracetamol or codeine should be taken with NSAIDs (unless contra-indicated) such as ibuprofen- which is also an anti inflammatory drug. If the pain killers you have been given are not sufficient please contact your consultant's secretary or your GP. The little incisions are covered with a small sticky dressing which should be kept dry and replaced with spare dressings when necessary. You will be given these before leaving hospital. You will be given a sling which will protect your shoulder and help with pain relief.
You will need a dedicated physiotherapy program after your surgery. If you have been seeing a physiotherapist prior to your surgery (who may have referred you to Guildford Upper Limb), you should arrange to see them afterwards so you can start your rehabilitation straight away. If you do not have a physiotherapist we can arrange one for you.
When can I return to driving and work?
If comfortable and feel able you can return to driving at 1 week.
You can return to a sedentary job as soon as you feel able, most patients return to light manual work at 3 weeks and heavy labour at 6 weeks. As a guide swimming and golf is 3 weeks and contact sports 6 weeks.