Acromio-clavicular Joint
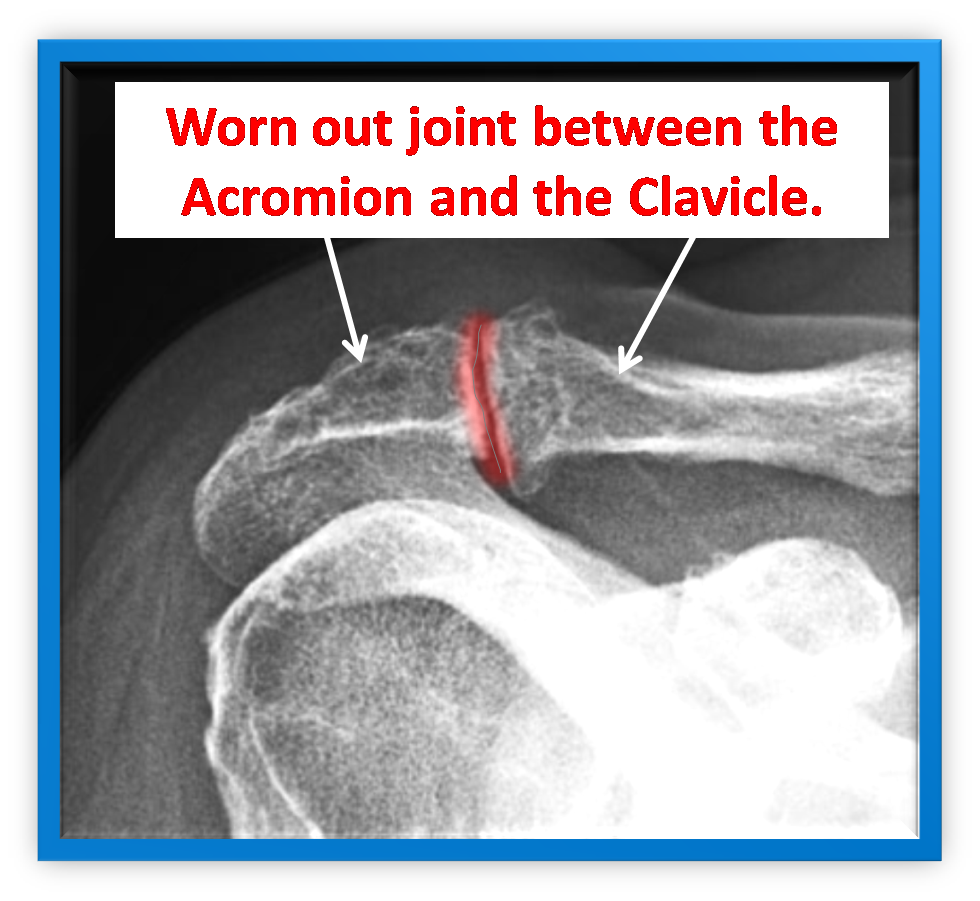
The small bony lump on the top of your shoulder is the acromio clavicular joint (ACJ). It's where the collar bone (clavicle) meets the top part of the shoulder blade (acromion). Several ligaments hold the joint in place.
Over time, the bones of the joint can wear out, become larger, and develop spurs around the joint. This can then result in a degenerative disease known as osteoarthritis. The diseased bone can then cause damage to the joint ligaments. The cushioning membrane within the joint (the bursa) can also become inflamed and thickened, causing pressure and inhibiting movement of the joint.
People who use their arms for extended periods of time (especially constant overhead lifting) are susceptible to ACJ arthritis. Another cause is an old injury, such as ACJ dislocation. Any activity that can put pressure on the joint (throwing sports, racquet sports, swimming etc) may eventually cause arthritis, too.
How do I know if I have ACJ arthritis?
You may notice a weakness in the upper arm and an aching pain on performing overhead activities. There may also be swelling in the joint as it is used. It can disrupt sleep, especially if you turn to lie on the affected shoulder.
If you're over 40, the symptoms above are good indicators of ACJ osteoarthritis. X-rays will show the degeneration of the bone. An MRI scan may be used to rule out or highlight other problems such as tendon or ligament tears. Arthroscopic diagnosis will clearly show whether you have degeneration of the bone.
What are the non surgical options?
Rest, analgesia and avoiding activities which make it worse. If these fail to control the pain and loss of function; the next step is an injection of steroid and local anesthetic into the joint. This can be very effective in relieving pain as the hydrocortisone acts as a powerful anti inflammatory.
| Information on hydrocortisone injections. After the injection the joint should be rested for 24 hours and the sticky plaster should remain on to prevent anything from entering the puncture site. Very rarely problems can occur with steroid injections- When the local anesthetic has worn off (about 4 hours), a few patients experience some pain, this will decline over a day or two. If you are diabetic your blood sugars should be monitored for the 6 hours following the injection. Infection is very rare and is reported to occur in 1 in 15000 patients. The skin overlying the injection site can become pale and thin, this is called lipodystrophy. |
The steroid injection works to mask the symptoms of the arthritis. It tends to work for 3-12 months but in some patients it hardly helps at all. In this situation surgery should be considered.
What is done at surgery?
After a routine shoulder diagnostic arthroscopy a shaver is introduced into the sub acromial space. If there is osteoarthritis in your acromio clavicular joint, it is necessary to shave the end of the clavicle - this is called a resection arthroplasty. During the arthroscopic surgery the thickened cushioning tissue (bursa) is removed, and any badly damaged ligaments will also be removed. The last 1cm of the collar bone will be cut off, and any bone spurs or diseased bone will be trimmed and smoothed out.The surgery is done with an anaesthetic block so the arm will be numb, if you prefer you can be awake during the operation or have some sedation to make you sleepy. Because the operation uses water to see inside the joint the wounds will leak a little fluid which will be absorbed by cotton wool dressings, which are removed a few hours after surgery. You can go home the same day after seeing the ward physiotherapist who will give you exercises to do. see video- excision distal clavicle.
What should I expect during recovery?
 Once the numbness has worn off (4-8 hours) the shoulder will become painful after the operation if you do not take regular pain killers as soon as you get home. Even though you may be pain free at rest you must take the tablets for when you move the shoulder as part of your rehabilitation program. A combination of regular painkillers such as paracetamol or codeine should be taken with NSAIDs (unless contra-indicated) such as ibuprofen- which is also an anti inflammatory drug. If the pain killers you have been given are not sufficient please contact your consultant's secretary or your GP. The little incisions are covered with a small sticky dressing which should be kept dry and replaced with spare dressings when necessary. You will be given these before leaving hospital. You will be given a sling which will protect your shoulder and help with pain relief.
Once the numbness has worn off (4-8 hours) the shoulder will become painful after the operation if you do not take regular pain killers as soon as you get home. Even though you may be pain free at rest you must take the tablets for when you move the shoulder as part of your rehabilitation program. A combination of regular painkillers such as paracetamol or codeine should be taken with NSAIDs (unless contra-indicated) such as ibuprofen- which is also an anti inflammatory drug. If the pain killers you have been given are not sufficient please contact your consultant's secretary or your GP. The little incisions are covered with a small sticky dressing which should be kept dry and replaced with spare dressings when necessary. You will be given these before leaving hospital. You will be given a sling which will protect your shoulder and help with pain relief.
You will need a dedicated physiotherapy program after your surgery. If you have been seeing a physiotherapist prior to your surgery (who may have referred you to Guildford Upper Limb), you should arrange to see them afterwards so you can start your rehabilitation straight away. If you do not have a physiotherapist we can arrange one for you.
When can I return to driving and work?
If comfortable and feel able you can return to driving at 1 week.
You can return to a sedentary job as soon as you feel able, most patients return to light manual work at 3 weeks and heavy labour at 6 weeks. As a guide swimming and golf is 3 weeks and contact sports 6 weeks.