Distal Radio-Ulna Joint Arthritis
Anatomy
There are 2 bones in the forearm; the radius and the ulna. At the wrist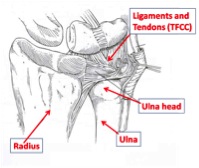 the hand is attached to the radius and it rotates around the ulna at the distal radio-ulna joint.
the hand is attached to the radius and it rotates around the ulna at the distal radio-ulna joint.Arthritis occurs when the cartilage which lines the joints is worn away and is found in any joint of the body. The joint in the wrist which allows you to rotate the forearm is called the distal radio-ulna joint or DRUJ and can be subject to arthritis. Symptoms are increasing pain, stiffness and mild swelling. It is usually due to instability or an injury from years before.
What are the non operative treatments?
The wrist can be rested in a splint and analgesia can improve the pain. The splints tend to restrict movement and are not well tolerated. Steroid injections can give good relief, but need to be given under x-ray control. Information on hydrocortisone injections. After the injection the joint should be rested for 24 hours and the sticky plaster should remain on to prevent anything from entering the puncture site. Very rarely problems can occur with steroid injections- When the local anesthetic has worn off (about 4 hours), a few patients experience some pain, this will decline over a day or two. If you are diabetic your blood sugars should be monitored for the 6 hours following the injection. Infection is very rare and is reported to occur in 1 in 15000 patients. The skin overlying the injection site can become pale and thin, this is called lipodystrophy.
What are the operative treatments?
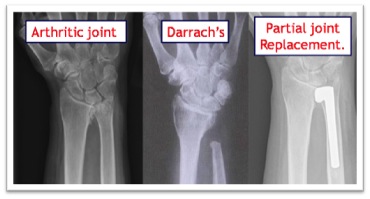
Darrachs . When rheumatoid arthritis affects the DRUJ the ulna head dislocates from the wrist joint and develops a painful lump on the back of the wrist. This can rub on the finger tendons as they pass over the wrist and are at risk of snapping. In rheumatoid arthritis the surgery is aimed at removing the worn out bone which removes the insult on the tendons and the painful arthritic joint. This is called a Darrachs procedure and gives good relief of pain.
Joint replacement . If the arthritis occurs in a younger or high demand patien
 t a joint replacement gives better results than removing the ulna head. This is because a Darrachs procedure in these patients can result in pain when gripping and carrying things as the stump of the remaining ulna bangs into the radius bone.
t a joint replacement gives better results than removing the ulna head. This is because a Darrachs procedure in these patients can result in pain when gripping and carrying things as the stump of the remaining ulna bangs into the radius bone. Only half of the ulna head is involved in the joint itself, the other half has ligaments an
 d tendons attached which are vital for stability of the joint. Recent advances in joint replacement mean that only the worn half of the head is replaced, leaving the ligaments and tendons alone to assist in the proper function of the wrist.
d tendons attached which are vital for stability of the joint. Recent advances in joint replacement mean that only the worn half of the head is replaced, leaving the ligaments and tendons alone to assist in the proper function of the wrist. The operation is indicated when all non operative measures have been exhausted. An 8cm incision is made in the back of the wrist and the soft tissues are carefully preserved. The stem is placed down the shaft of the bone which fixes it in firmly. The soft tissues are then repaired over he top and skin stitched with absorbable sutures. A small sticky dressing or gauze is used to keep the wound clean and dry. A plaster is applied to protect the joint replacement while the tissues around it heal.
What to expect after surgery?
The wrist will have local anesthetic injected into it at the end of the operation; this will make it numb. At 2-6 hours the wrist will become painful and regular pain killers should be taken straight away, do not wait until the wrist becomes uncomfortable. The hand must be elevated to reduce swelling and bleeding, both of which will turn to scar tissue and prolong the recovery. The fingers should be moved to stop stiffness. The plaster will be replaced with a light weight splint at 2-7 days after surgery; this will be arranged for you after discharge form hospital. The wound will heal at 2 weeks and can be allowed to get wet at this stage. The removable splint must be worn for 6weeks because the wrist must remain in a certain position while the soft tissues heal. The hand should not be turned downwards for 6 weeks, if it is allowed to rotate downwards (pronation) too early; the ulna head replacement may become unstable.When can I get back to work?
Return to driving at 6 weeksReturn to work will depend on your occupation.
- Office based work which can be performed with one hand can be started as soon as you are comfortable.
- Office work which requires both hands at 6-8 weeks and manual work at 12 weeks.
Heavy manual occupations and hammering movements should be discouraged to protect the implant from loosening and/or dislocation in the future.
Post-operative Management Guidelines for your therapists
Where stiffness is likely:- i.e. revision surgery for failed Darrachs or Sauve-Kapanje procedure
- Sugar Tong plaster of Paris is applied after surgery and converted to a sugar tong splint as comfort and oedema dictate
- Mobilisation of the DRUJ commences at 2 weeks but not pronation.
- Active and passive exercises
- Support the joint in a splint, for comfort, between exercises and to protect against forced rotation.
- A Sugar Tong POP to control forearm rotation is applied in theatre and converted to a Sugar Tong splint as comfort and oedema dictate.
- A clinical and radiological assessment is carried out at 6- weeks.
- If x-ray satisfactory and implant stable rotation block splinting can be discarded and unrestricted mobilisation commenced. If necessary, for comfort, or concerns related to heavy activity, a removable below elbow splint should be provided.
- If instability is still likely to occur controlled mobilisation, within the limits of stability, is commenced and a sugar tong (or substantial below elbow splint) retained for between exercise and at night. This is discarded when stability is achieved.
- When movement potential has been maximised strengthening exercises are encouraged.
?