Abstract Boston, USA
Pyrocarbon PIPJ arthroplasty
Anthony Hearnden
MATERIAL
Pyrolytic carbon material was first used as an implanted mechanical heart valve device by Dr Gott in 1966. He demonstrated its low friction properties and confirmed that it was an inert material which was suitable as a biological implant (haubold 1994). A graphite rod is precision machined to form the core shape of the implant. The rod is 1% tungsten which is radio-opaque meaning it can be seen on x-ray. It is then coated with the pyrolytic carbon (Pyro = heat and lysis=break apart) using a chemical vapour deposition process. Hydro carbon gas (methane) is heated to 1300oC which breaks apart the carbon-hydrogen chemical bond. The graphite implant which is suspended in the jet of the super heated methane is coated in the pyrolytic carbon. The pyrolytic coating has no tungsten in it and is therefore radiolucent; giving the characteristic appearance of lucency on the follow up x-rays. The articular surface is then polished and is ready for sterilisation.
ADVANTAGES
Pyrolytic carbon has properties which, according to our current understanding of material science, offer an advantage over other materials when applied to arthroplasty. It is chemically inert; there are no metallic ions or problems with oxidation. It has an elastic modulus similar to cortical bone Ey= 3 x106, giving it biomechanical compatibility and stops stress shielding. It exhibits isotropic properties, made from a continuous structured layer of homogeneous carbon and is not a carbon fibre. It does not exhibit fatigue failure and has a high wear resistance; pyrocarbon has properties of both 2 dimensional and 3 dimensional structures resulting in strength and wear properties lying between those of graphite and diamond. Experience in its use at the mcpj (Bravo,Cook) has demonstrated it to be an effective material when used for arthroplasty in the hand.
Uncemented and no polyethylene; the pyrocarbon PIPJ is press fit into the bone of the phalanges. There is no cement or polyethylene, both of which are associated with third body wear, osteolysis and subsequent loosening.
Unhinged implant; I cannot think of anywhere in the body that a hinged implant has not been tried, failed and then superseded with an unlinked implant. Linked implants have a clear role in low demand patients with poor quality tissue and unstable joints such as rheumatoid arthritis. However in high demand patients, such as those with osteoarthritis, loosening of hinged implants has been a problem (swanson). The link results in all the forces being transferred directly to the bone/cement/implant interface. The pyrocarbon implants are a bicondylar, semi-constrained articulation where the soft tissues which can absorb some of the energy.
Able to withstand coronal forces; the collateral ligaments are preserved and the pyrocarbon is not compressible, the PIPJ is able to withstand greater forces reducing coronal angulation, which allows an increased grip strength. (Branam 2007). This is particularly important in the index finger where silastic implants allow little functional pinch grip.
DISADVANTAGES
Initially it was thought that bone was able to osteo-integrate with pyrocarbon. However in vivo studies have shown it not to be the case (Daecke). Radiological appearances of the line of sclerosis around the stem have heightened concern over the way in which it is fixed into the bone (Herren). It is reported that bone will 'on grow' to pyrocarbon because the modulus of elasticity is close to that of bone. This is a new way of a material interacting with bone and there are no long term follow up studies in the PIPJ . There are reports that there can be a period of settlement of the stem into the shaft (Bravo). The Wrightington PIPJ experience, some with a follow up of 9 years, suggests that pyrocarbon will sit in bone for many years without moving. Our experience of removing PIPJ implants is mixed; some come out very easily and others are so well fixed an osteotomy of the phalynx has been required.
Cost- Compared with silastic or a PIPJ fusion, the pyrocarbon arthroplasty is expensive. Like other implants it is 2-3 times more expensive.
REVIEW OF LITERATURE
Table 1. is a summary of the results of the published literature. The results from the 97 PIPJ replacements performed at our institution have been added.
Year | Author | Number | m/f | F/U months | Age | Increase arc | Re-operation | Revision | satisfaction | Pain |
2006 | Branam | 19 | 00:10 | 19 (6-36) | 62 (52-69) | 1 | 0 | 81% | 2 | |
2006 | Herren | 17 | 10 (12_27) | 64 (55-81) | 8 | 6% | 6% | 71% | 8 to 1 | |
2006 | Nunley | 7 | 02:03 | 17(12-23) | 40 (28 -56) | -2 | 28% | 28% | 14% | 6 to 4 |
2007 | Ng | 15 | 02:12 | 27.4 (7-44) | 62 (38-82) | 15.3 | 20% | 0 | 8 to 2 | |
2007 | Bravo | 50 | 15:20 | 37 (27-46) | 53 (21-73) | 7 | 28% | 8% | 80% | 6 to 1 |
2010 | Ulrika Wijk | 53 | 07:36 | 24 (12-60) | 59 (40-85) | -8 | 13% | 2% | 3 to 0.4 | |
2010 | Watts | 97 | 21:51 | 56 (24-108) | 56 (24-79) | 13 | 13% | 76% | 2 |
Pyrocarbon PIPJ replacement offers effective and reliable pain relief.
As with other types of implant the increase in range of motion is modest. When the PIPJ has been stiff for a long time the introduction of an implant into the joint will not improve its range of motion. This surgery should only be performed for pain and patients must be counselled regarding the range of motion.
The post operative early complications are more frequent when compared with silastic implants (Branam, Bravo). Reviewing the 259 cases published in the literature; there have been 80 complications reported -24%, many leading to further surgery. Some complications are mild such as squeaking but others are more serious. Stiffness is the most common (11%), Swan neck deformity (4%), instability (3%), Pain (2%), operative fracture (2%), Infection (1.5%) and loosening (1%).
Revision rate for all reported cases, however is only 8%.
OUR EXPERIENCE
Satisfaction.
· 76% said they would have the same operation again
· The median satisfaction score was 2/10 = very satisfied.
Range of motion.
· No significant difference in pre and post op range of movement (Wilcoxon Signed Ranks Test p = 0.174 for arc)
· Significant correlation between pre-operative extension and post-operative extension Spearman's rho = 0.48, p = 0.004
· There was no significant difference in outcome on any measure between those having a central split dorsal approach and those having a chamay approach.
Revision.
· Revision rate 13% at a median time of 15 months (IQR 4-27)
· A Kaplan Meier survivorship curve of 97 pyrocarbon proximal interphalyngeal joint replacements with a mean follow up of 5 (2-9) years demonstrates an 85%, nine year survival.
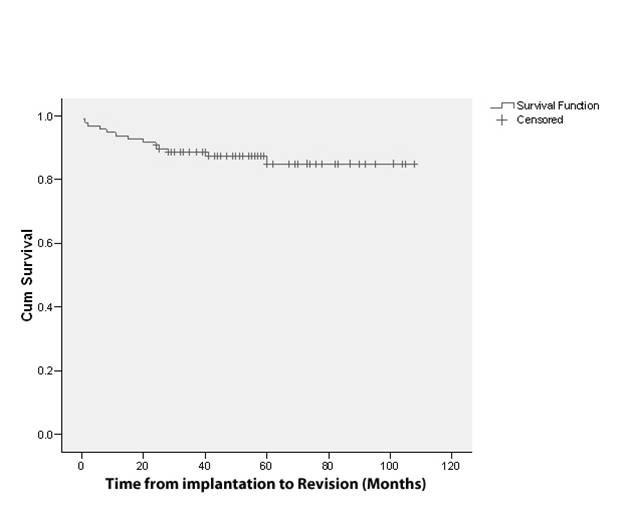
· Reasons for revision were; Instability (7%) Aseptic loosening (3%) stiffness (2%) and infection (1%).
· Ten percent of all implants were revised within 2 years of surgery (77% of all the revisions). Interestingly after the first 2 years, the pyrocarbon appears to exhibit excellent survival.
PIPJ replacement surgery is technically difficult and while the implant is capable of long survivorship it is uncompromising. These first 97 PIPJ arthroplasty represent our learning curve and our conclusions are listed bellow as Tips and Tricks.
TIPS AND TRICKS
ü Patients with inflammatory disorders or collateral ligament insufficiency are poor candidates.
ü The integrity of the PIPJ collateral ligaments must be preserved, if they become damaged reinforcing with a 'collateral stay stitch' can be effective. When in doubt convert to a silastic implant or fuse the joint; instability is certain with no collaterals.
ü Patient expectations must be addressed regarding modest improvement in range of motion.
ü Care must be exercised to preserve the insertion of the central slip. The Chamay approach requires careful repair of the extensor mechanism to allow early rehabilitation.
ü Early indications are that the lateral approach, which leaves the central slip untouched, may afford earlier rehabilitation and greater range of motion.
ü Osteotomy for the distal component requires removal of only a small amount of bone. In many instances this can be accomplished with a burr. Too much leads to swan necking.
ü Consider the flexion/extension gaps. Taking more bone off the proximal phalynx will increase the extension gap alone, while more bone off the distal phalynx will increase both flexion and extension gaps. Implants which are too tight (over stuffed) are a leading cause of stiffness.
ü The distal component must go in the right way round. Unlike the tibial component in the knee, the hollowed surface fits under the central slip.
ü Use a burr and fluoroscopy to fit the largest size possible. Under sizing the implant may result in subsidence, instability and posterior cortical impingement.
ü Use fluoroscopy frequently as mal alignment will lead to an imbalance in the forces acting across the joint resulting in worsening angulation and failure.
ü The proximal osteotomy must not be too acute an angle; excising too much volar cortex will lead to flexion of the implant.
ü If hyperextension is present after surgery it must be addressed early in the rehabilitation. A 45 degree extension blocking splint worn for 3 weeks.
S.D. Cook, R.D. Beckenbaugh, J. Redondo, L.S. Popich, J.J. Klawitter and R.L. Linscheid, Long-term follow-up of pyrolytic carbon metacarpophalangeal implants, J Bone Joint Surg 81A (1999), pp. 635-648.
W Daecke, Veyel k, Wieloch P, Jung M, Lorenz H, Martini AK. Osseointegration and mechanical stability of pyrocarbon and titanium hand implants in a load-bearing in vivo model for small joint arthroplasty. J hand Surg 2006;31A:90-97.
C.J. Bravo, M. Rizzo, K. Hormel and R.D. Beckenbaugh, Pyrolytic carbon proximal interphalanegal Joint arthroplasty: results with minimum two-year follow-up evaluation, J Hand Surg 32A (2007), pp. 1-11.
R. Meier, M. Schulz, H. Krimmer, N. Stutz and U. Lanz, Proximal interphalangeal joint replacement with pyrolytic carbon prostheses, Oper Orthop Traumatol 19 (2007), pp. 1-15.
H.G. Tuttle and P.J. Stern, Pyrolytic carbon proximal interphalangeal joint resurfacing arthroplasty, J Hand Surg 31A (2006), pp. 930-939.
D.B. Herren, S. Schindele, J. Goldhahn and B.R. Simmen, Problematic bone fixation with pyrocarbon implants in proximal interphalangeal joint replacement: short-term results, J Hand Surg 31B (2006), pp. 643-651.
Swanson S.B, Maupin B.K, Gajjar N.V, Swanson G.D. Flexible implant arthroplasty in thr proximal interphalygeal joint of the hand. J Hand Surg 1985:10A796-805.